Bioinformatics, Epidemiology, and Lp(a) Center for Research and InnOvatioN
Scientific Background
Learn how Lp(a) affects heart health.
Clinical practice should change
While much progress has been made in monitoring and lowering LDL-C, there are other biomarkers that need to be targeted and residual risk for cardiovascular disease can be lowered.
Lipoprotein(a) (abbreviated Lp(a)) is an LDL-like particle with other moieties that make it more pro-atherogenic, pro-inflammatory, and anti-fibrinolytic.
One in five people have significantly elevated Lp(a). Because it is so common and harmful, this is a biomarker that should not be neglected.
Watch Dr. Taub try to convince clinicians to change their clinical practices regarding Lipoprotein(a) at the Complex Coronary Cases (CCC) 2023 conference.
Lp(a) in Focus: Current Knowledge & Approach to Patient Care
Presenter: Michael Wilkinson, MD, FACC, FNLA
We have learned a great deal about lipoprotein(a), but there is much more to discover.
Watch Dr. Michael Wilkinson, Associate Professor of Medicine and Director of the Advanced Lipid Disorders Treatment Program at UC San Diego Health, discuss the current knowledge and provide an approach to caring for patients with elevated lipoprotein(a).
New Evidence
• Data continue to accumulate from large, population-based studies indicating that elevated plasma Lp(a) is an important risk factor for atherosclerotic CVD and calcific aortic valve disease
• The available clinical evidence allows for a more precise model of how to incorporate Lp(a) levels into clinical decision-making
• There have been important advances in understanding of the genetic basis for variation in Lp(a) levels, and with them has come further evidence for the causality of elevated Lp(a) in CVD
A Focused Update to the 2019 NLA Scientific Statement on Use of Lipoprotein(a) in Clinical Practice
Overview: The lipoprotein(a) [Lp(a)] field is rapidly evolving on many fronts, including understanding of the association between Lp(a) levels and cardiovascular disease (CVD) risk in different contexts, and how best to manage other CVD risk factors in patients with elevated Lp(a). Considering new insights into the clinical management of these patients, and in the absence of FDA-approved therapies to specifically lower Lp(a) levels, the question of in whom Lp(a) should be measured has become an increasingly important issue in clinical practice.
Authors: Marlys Koschinsky, PhD, Archna Bajaj, MD, MSCE, Michael Boffa, PhD, Dave Dixon, PharmD, CLS, FNLA, Keith Ferdinand, MD, Samuel Gidding, MD, Edward Gill, MD, Terry Jacobson, MD, MNLA, Erin Michos, MD, MHS, Maya Safarova, MD, PhD, Daniel Soffer, MD, Pam Taub, MD, Michael Wilkinson, MD, Don Wilson, MD, Christie Ballantyne, MD
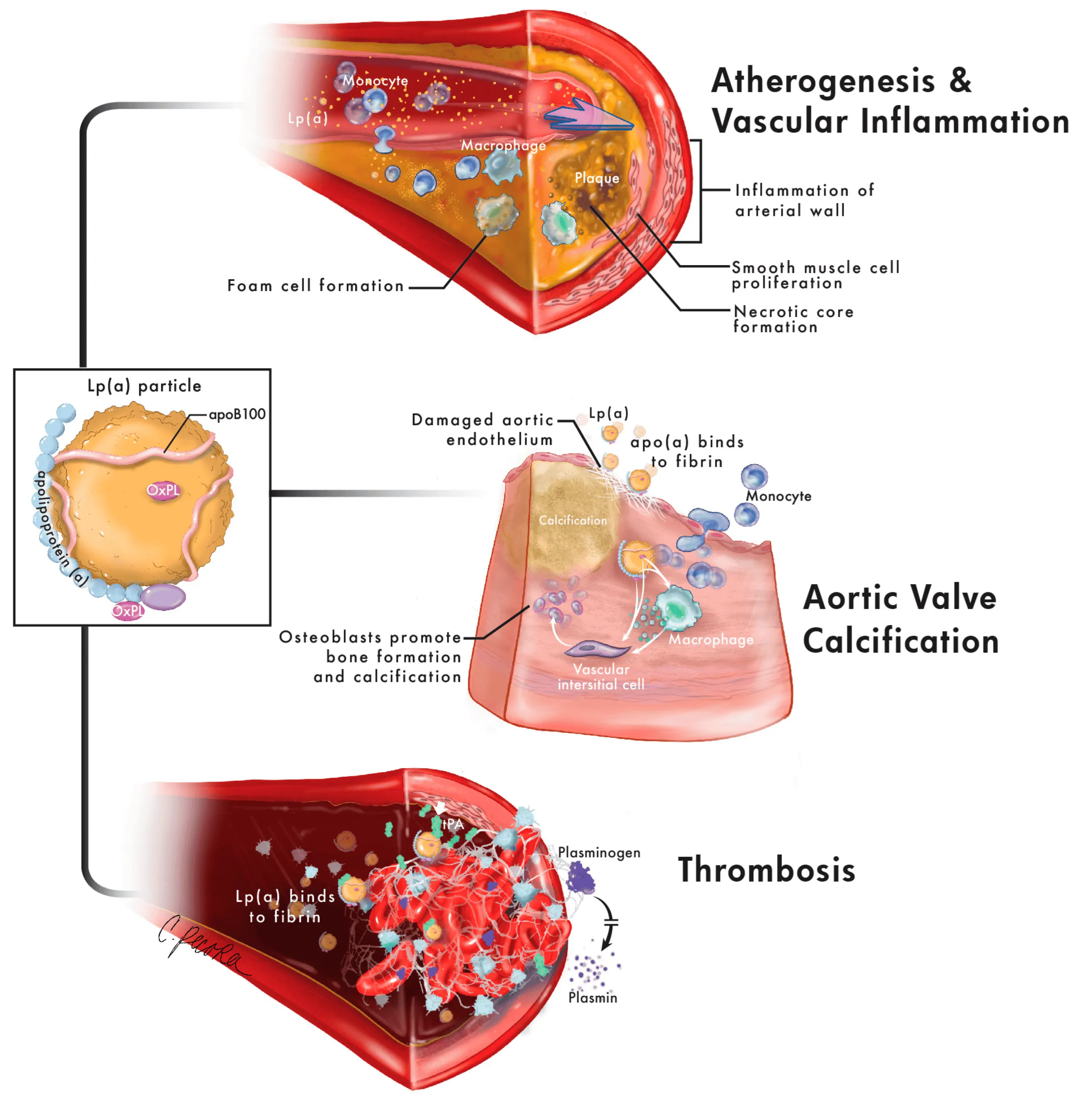
Mechanisms of cardiovascular risk related to Lp(a)
Lipoprotein(a) and its individual components are associated with cardiovascular disease through multiple overlapping mechanisms.
Lp(a) is composed of apolipoproteinB100 (apoB100) and apolipoprotein(a) (apo(a)), both of which contain oxidized phospholipids (OxPL).
The apoB100 contributes to atherogenesis through similar mechanisms as low-density lipoprotein (LDL), including vessel wall binding, smooth muscle cell proliferation, foam cell formation and necrotic core formation.
OxPL contribute to vascular inflammation through increased transmigration and cytokine production by monocytes as well as upregulation of inflammatory genes.
Lp(a) contributes to aortic valve calcification as apo(a) binds to fibrin on injured aortic endothelium, and OxPL promote calcification and bone formation via vascular interstitial cells and upregulation of reactive oxygen species and proinflammatory cytokines in macrophages.
Finally, apo(a) contributes to thrombosis by inhibiting fibrinolysis through competitive inhibition of tissue plasminogen activator (tPA) activation of plasminogen to plasmin and plasminogen binding to fibrin as well as promoting increased platelet activity.
Bhatia, H.S.; Wilkinson, M.J. Lipoprotein(a): Evidence for Role as a Causal Risk Factor in Cardiovascular Disease and Emerging Therapies. J. Clin. Med. 2022, 11, 6040. https://doi.org/10.3390/jcm11206040
Clinical guidelines and consensus statements recommend screening for Lp(a)
Clinical guidelines and consensus statements recommend screening for Lp(a): When, in whom, and why? Multiple global clinical guidelines and expert consensus statements recommend Lp(a) screening to manage dyslipidemia and mitigate Lp(a)-mediated CVD risk.
Provided is a synopsis of key recommendations for measuring Lp(a) from the: American Heart Association/American College of Cardiology (AHA/ACC), Canadian Cardiovascular Society, and European Society of Cardiology/European Atherosclerosis Society (ESC/EAS) clinical guidelines; and the ACC, American Association Clinical Endocrinology/American College of Endocrinology (AACE/ACE), EAS, and National Lipid Association (NLA) consensus statements.
*Denotes clinical guideline; †Denotes scientific/consensus statement; ‡Premature atherosclerotic cardiovascular disease (ASCVD) is defined as occurring in men aged <55 years and women aged <65 years.